The first report of severe Haemophilia A in combination with spontaneous internal carotid artery dissection
1. Case Discussion
A 57 year old man presented to the haematology day unit after self-reporting an abnormality with his pupils. He described how he had woken up on the morning of his presentation with his right pupil being larger than his left. On further questioning he also described a dull, gradual onset, relatively mild left sided temporal headache.
He did not report any trauma to the head or neck preceding his symptoms. He denied any visual disturbances and had no constitutional symptoms. His past medic al history include severe haemophilia A for which he self-administers the recombinant coagulation factor eight (Refacto AF, Moroctocog alfa) product at a dose of 1000 IU on alternate days. He also had severe haemophiliac arthropathy. He had no additional medical problems, no known risk factors for vascular disease and no known collagen vascular disorders. He was not taking any other medications, was a non-smoker and denied illicit drug use. There was no family history of vascular disorders or strokes.
On examination he was comfortable, alert and orientated. Glasgow Coma Score (GCS) was 15/15. Neurological examination revealed no limb or obvious facial weakness. Further examination however revealed a left sided constricted pupil and a mild left sided ptosis without anhidrosis - Horner's syndrome (the absence of anhidrosis i.e. incomplete Horner's, is suggestive of a post ganglionic lesion). He was haemodynamically stable with a blood pressure of 128/75 and a heart rate of 80 beats per minute. The combination of a Horner's syndrome and left sided headache raised the possibility of internal carotid artery dissection.
2. Investigations
Patient's full blood count and renal function were normal. His clotting results and Factor VIII levels were as follows:
- INR: 0.9
- PT: 12.7 seconds (11s-15s)
- APTT: 41 seconds (25s-35s)
- Factor VIII level: 24.0 IU/ml (50-150)
- Factor VIII Inhibitor: <0.4 Bethesda
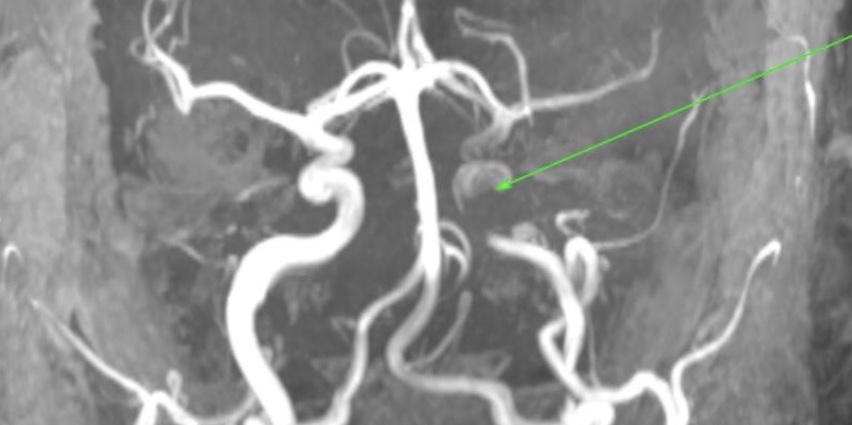
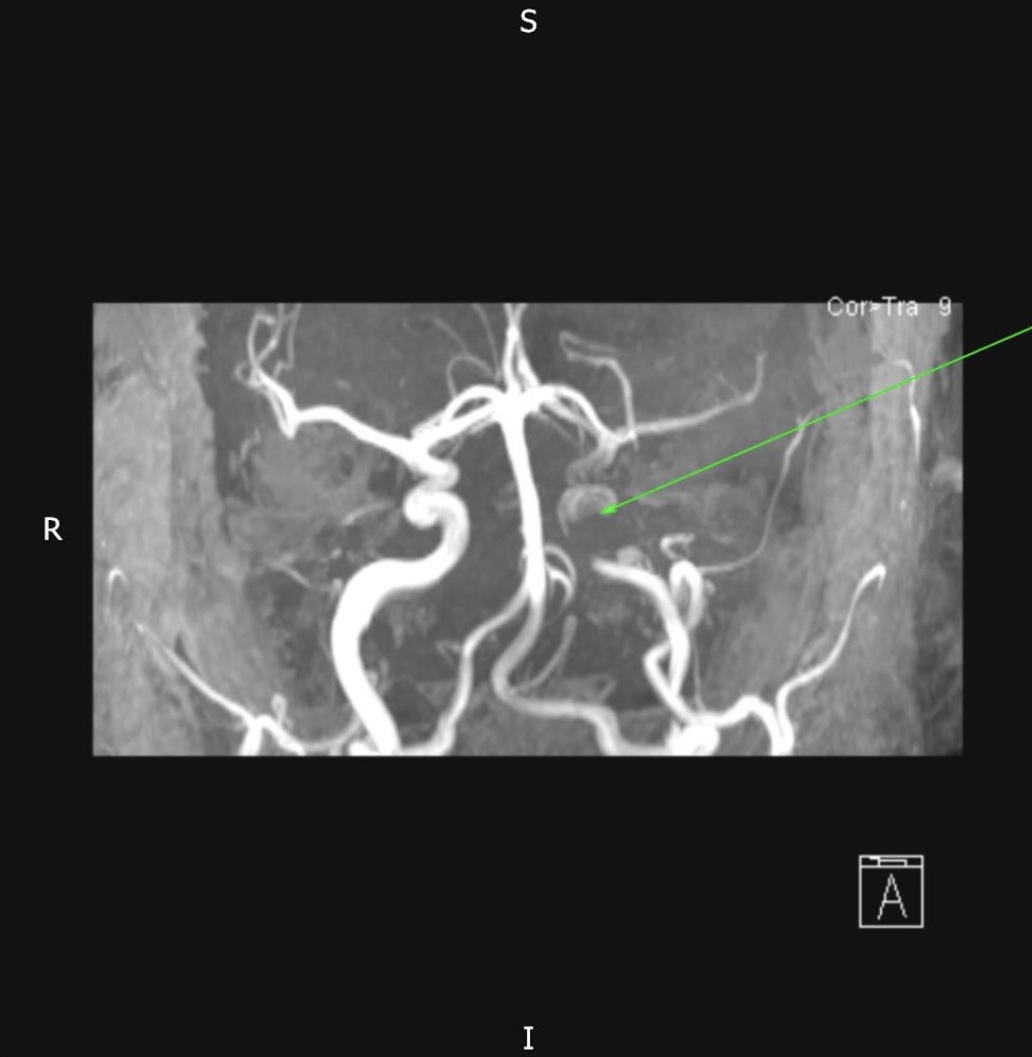
Computed tomography (CT) brain was normal. Magnetic resonance imaging (MRI) brain, magnetic resonance angiography (MRA) brain and MRA both carotids were subsequently undertaken and revealed a left internal carotid artery dissection (Figure 1) with no evidence of cerebral infarction or haemorrhage. A subsequent ultrasound Doppler of the carotid arteries characterised the lesion to be at least 2.2cm of the distal left internal carotid artery.
3. Differential diagnosis
The presence of a new onset Horner's syndrome opens up a wide variety of differential diagnoses. Ranging from bronchogenic carcinoma (Pancoast tumour) and migraine to brain tumours and traumatic causes. The presence of a temporal headache in combination with the new abnormal neurological finding led us to investigate the carotid arteries for dissection. It is certainly important to consider this diagnosis in patients with unilateral abnormal neurological signs with the addition of unilateral pain.
4. Treatment
Prevention and treatment of ischaemic insult to the brain is the primary management goal in patients with carotid artery dissection as the dissecting lumen (false lumen) can become thrombosed and lead to complete occlusion of the carotid artery. For this reason anticoagulation and anti-platelet treatment is widely advocated to be beneficial - primarily based on its biological plausibility and from clinical experience.
However, Lyrer et al. have conducted a Cochrane review of management of patients with carotid artery dissection and found that no randomised controlled trials have yet been conducted to establish which treatment modality (anticoagulation or anti-platelet - if any) is superior [1]. Multiple cohort studies have suggested that anti-platelet treatment and anticoagulation have equal efficacy when death or disability are used as endpoints [2].
However in patients with severe haemophilia the risk of bleeding is significant if anticoagulation is introduced. Very little literature is available to guide management in these patients and clinicians must therefore rely on expert opinion.
In this patient we decided to initiate anti-platelet treatment. He was loaded with 300mg aspirin and then commenced on 75mg of aspirin once daily. Prior to loading with aspirin he received 3000 IU Refacto AF (Recombinant Factor VIII) and confirmation that his Factor VIII levels were 100% of normal was checked prior to treatment. He remained on Refacto 3000 IU once daily with daily 'trough' factor VIII level monitoring. We aimed for a Factor VIII level of 100% initially.
The patient remained an inpatient for 5 days for treatment and monitoring. The possibility of endovascular repair and stenting was raised with the vascular surgeons and interventional radiologists however the dissection was not amenable to any surgical correction. He was discharged on aspirin 75mg once daily and Refacto 1000IU once daily - the aim was to ensure 'trough' Factor VIII levels remain approximately 20%.
5. Outcome and follow up
The patient remained well throughout his inpatient stay however he occasionally reported headaches. His Horner's syndrome partially resolved during his inpatient stay. We plan to follow him up closely in our Haemostasis Clinic and repeat an MRI of his carotid arteries in 3 months to assess the resolution of his dissection. We will continue to monitor his 'trough' Factor VIII levels as an outpatient and address any co-existing risk factors for cardiovascular disease.
6. Discussion
Whilst Gatti et al. (1996) have described a case of a haemophilic patient presenting with headache and Horner's syndrome [2] (with MRI showing carotid artery dissection) this is the first case to my knowledge in which active management was initiated and described (no therapy in this previous case).
The combination of these two clinical entities (haemophilia and carotid artery dissection) are likely to be extremely rare and this is the first reported case of its management.
Haemophilia A is a rare X-linked congenital bleeding disorder caused by a deficiency of coagulation Factor VIII [5]. It is characterised, in its severe form (clotting factor level $<$1 IU/dL), by spontaneous bleeds into joints and muscles. Management is complex and involves a multi- disciplinary approach. Anti-platelet medication and non-steroidal anti-inflammatory drugs (NSAID's) are generally avoided. Patients with Haemophilia A do develop cardiovascular disease and therefore these patients do develop an indication for anticoagulation or anti-platelet treatment. When these situations arise, management involves raising factor VIII levels and then initiating treatment.
A consensus review of the treatment of cardiovascular disease in people with Haemophilia A and B in 2015 [6] has previously suggested raising factor levels to at least 80% prior to emergency angioplasty for the treatment of ST elevation myocardial infarction and 100% prior to aortic repair. These values are suggested to be maintained for at least 48 hours.
The ADVANCE working group looking into the management of AF in patients with haemophilia have published a consensus view of leading European haemophilia centres on the use of anticoagulation and anti-platelet treatment for stroke prevention [5]. The opinion of this group was that only patients with very high CHADsVasc score should be managed with anticoagulation or anti-platelet treatment (with adequate Factor VIII replacement) and they also suggested a minimum trough level of 0.035 IU/ml for anti-platelet treatment and 0.24 IU/ml for anticoagulation treatment.
The rare combination described in this report (combination by chance rather than association) of a spontaneous internal carotid artery dissection in a patient with severe haemophilia A can be managed in a similar manner with adequate Factor VIII replacement followed by aspirin monotherapy.
In our case we decided to aim for a higher trough levels (100% initially and 20% thereafter on discharge) after discussion with the experts at the Oxford Haemophilia and Thrombosis Centre - who have significant experience in similar cases. In addition as a bleed at the site of dissection would be catastrophic for the patient a more cautious approach was adopted.
7. References
[1] Antithrombotic drugs for carotid artery dissection. The Cochrane database for systematic reviews. Lyrer P and Engleter S. 2003.
[2] Spontaneous Carotid Dissection in a Haemophilic Patient: MR and Angio-MR Findings. The Neuroradiology Journal. A. Gatti et al. 1996.
[3] Aspirin vs Anticoagulation in carotid artery dissection. Neurology - American Academy of Neurology. Georgiadis D et al. 2009.
[4] Guidelines for the management of haemophilia. Haemophilia. Srivastava A et al. 2013.
[5] Management of atrial fibrillation in patients with haemophilia - A consensus view by the ADVANCE working group. Schutgens REG et al. Haemophilia 2014.
[6] Consensus Review of the Treatment of Cardiovascular Disease in People With Hemophilia A and B. Cardiology in Review 23: 53-68. Ferraris et al. 2015.
- Log in to post comments










