Type 1 Cardio-renal Syndrome in Chinese Elderly: a case report

1. Case Illustration
1.1 Presenting complaint
An 81-year-old Chinese lady was admitted with shortness of breath since 3 days before admission from nursing home.
1.2 History of presenting complaint
An 81-year-old Chinese lady complained about worsening shortness of breath, paroxysmal nocturnal dyspnoea and dyspnoea at rest since 3 days before admission from nursing home. The symptoms were relieved by sublingual glyceryl trinitrate and oxygen.
1.3 Past medical history
This patient was known to have:
- Hypertension
- Hyperlipidaemia
- Diabetes mellitus
- Knee osteoarthritis
- Ischaemic heart disease (IHD)
- Anaemia of chronic disease
- Left central retinal artery occlusion
- Stage 4 chronic kidney disease (CKD)
- Vascular dementia
- Recurrent falls.
1.4 Drug history
There is no known drug allergy (NKDA). The patient’s regular medications are as follows:
- Furosemide 20mg PO OM
- Paracetamol 500 mg and Codeine 8 mg 1 tab PO TDS PRN
- Glyceryl trinitrate (GTN) 0.5mg sl PRN chest pain
- Atorvastatin 10mg PO ON
- Bisacodyl 10mg PR PRN no bowel movement for 2 days
- Lactulose 10ml PO TDS
- Sennosides 7.5mg 2 tab PO PRN
- Macrogol 4000 1 sachet PO BD
- Cholecalciferol (Vit D3) 1000 units PO OM
- Omeprazole 20mg PO OM
- Bisoprolol fumarate 5mg PO OM.
1.5 Physical examination
On examination, patient was afebrile. Blood pressure was 149/76, heart rate was 79 times/min, respiratory rate was 20 times/min, and SatO2 was 95%. Head and neck inspection, palpation and auscultation revealed no abnormal mass and inflammatory signs. Head and neck lymph node enlargement were absent. On examination of cardiovascular system, the jugular venous pressure (JVP) was elevated. Heart sound was normal, with no additional heart sound and murmur. On examination of respiratory system, trachea was not deviated. There were bibasal crepitations, reduced breath sound in lung bases and stony dullness on percussion on respiratory system examination. Abdomen is soft and non-tender with normal bowel sound. Liver, spleen and kidney were not palpable. There was pedal oedema up to the level of ankle. Sacral oedema was absent. Capillary refill time (CRT) was <2s.
2. Investigations
In A&E department, routine blood test and septic workup were done. Initial investigations revealed bilateral pleural effusion and blunted costophrenic angle on chest x-ray radiograph, see Figure 1. Electrocardiography (ECG) showed sinus rhythm with heart rate of 79 beats/minute due to beta-blocker and ST depression in lateral leads. Troponin-T level was 365 ng/L (compared with 41 ng/L in April 2018) and NT pro-BNP level was >35,000 pg/mL (compared with 3,812 pg/mL in April 2018). Full blood count (FBC) showed haemoglobin level of 9.9, total white blood cell count of 11.4, and platelet count of 135, which suggest anaemia and leucocytosis.
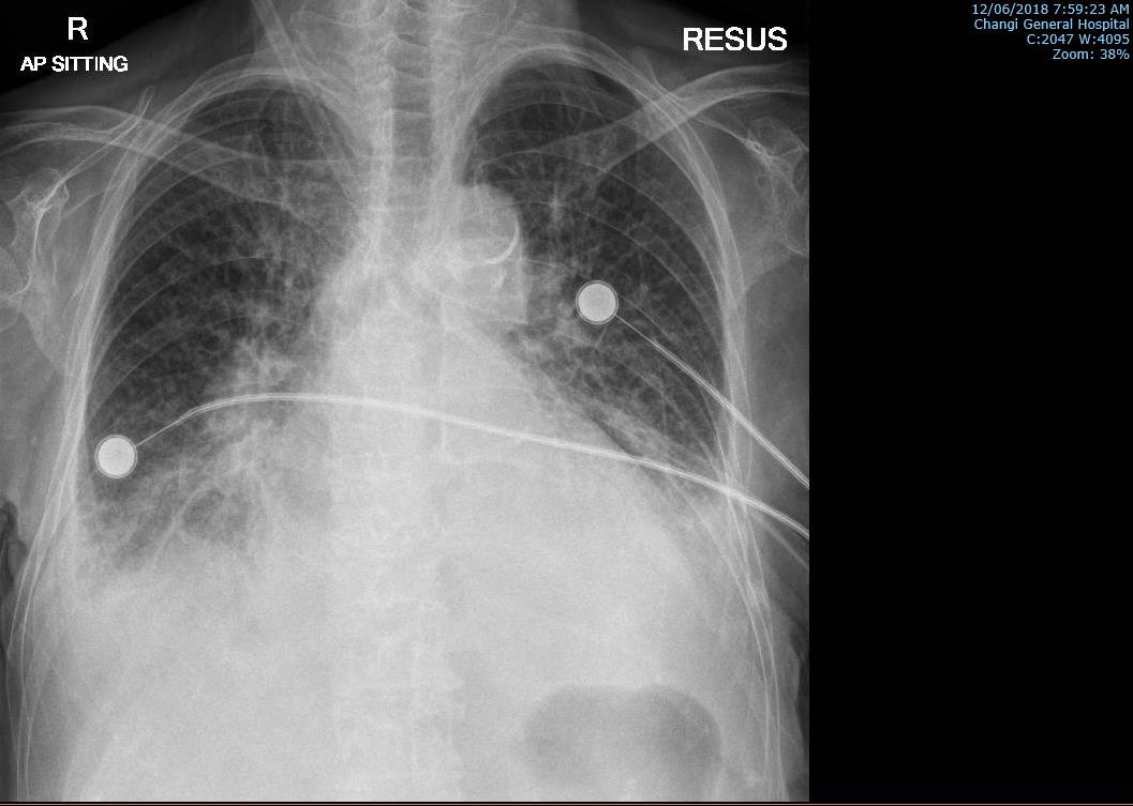
Figure 1: Chest x-ray radiograph at A&E showing bilateral pleural effusion.
3. Differential Diagnosis
- acute pulmonary oedema
- non-ST elevation myocardial infarction
- chest infection
4. Treatment
The following treatment was given in the A&E department:
- Furosemide 100mg IV
- Aspirin 100mg PO
- Clopidogrel 300mg PO
- GTN 0.5mg PO
- GTN patch 5mg
- 100% FiO2 with NRM
- Indwelling catheterisation.
On the ward, patient was observed to have delirium. Pittsburgh agitation score was 10, with remarkable scores in sleep disturbance and agitation domains.
Patient had daily weight measurement and sepsis workup was done. Fluid balance was monitored. Additional assessments include chest x-ray radiography, serum creatinine, serum urea, troponin-T, pro-calcitonin, and C-reactive protein levels, see Figures 2–8. Referral to physiotherapist (PT) and occupational therapist (OT) was made.
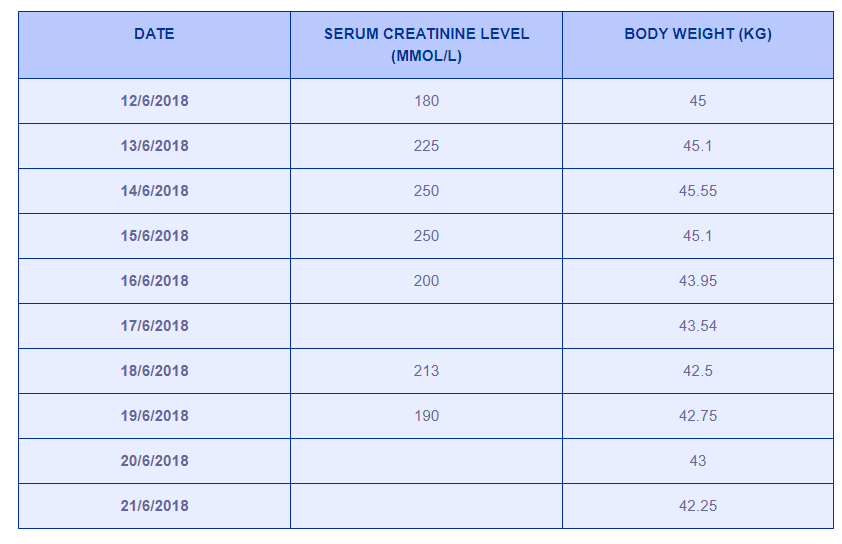
Table 1: Serum creatinine level and body weight measurement results.
Measurements of serum creatinine level and body weight over time can be seen in Table 1. The documented dry weight during the last discharge 4 months before current admission was 43 kg. NT pro-BNP level over time showed the level of >35,000 pg/mL at the beginning of observation and 30,318 pg/mL at the end of observation after treatment in the ward. Blood culture result was negative, whereas urinary culture showed mixed bacterial growth with >100,000 CFU/mL. This was not thought to be significant as the urine sample was taken from indwelling catheter (IDC).
In the ward, the patient was treated with furosemide 80mg IV BD, amiodarone HCl 200mg PO bid after detection of paroxysmal atrial fibrillation (AF), and sublingual GTN 0.5mg PRN chest pain.
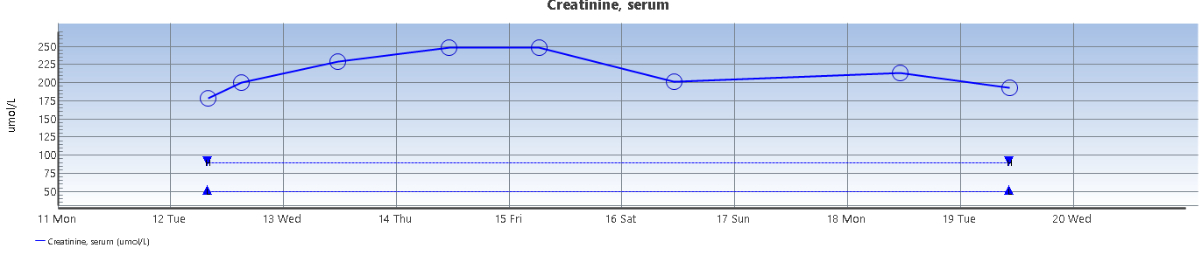
Figure 2: Serum creatinine level measurement results.
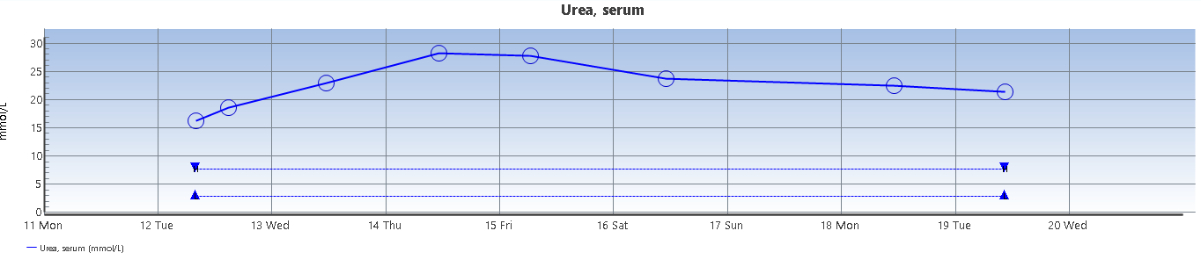
Figure 3: Serum urea level measurement results.
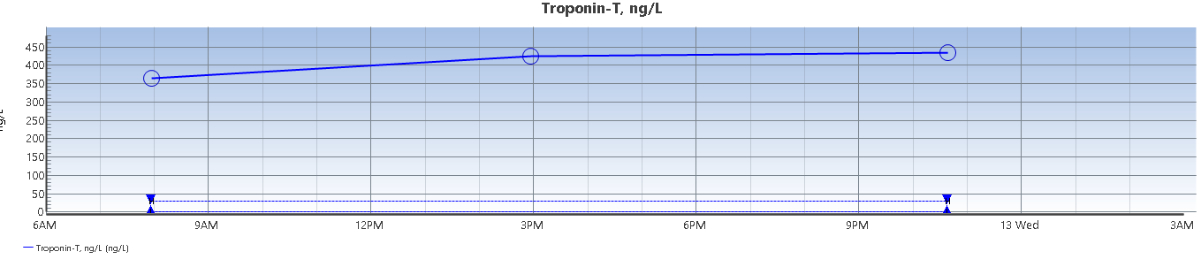
Figure 4: Troponin-T level measurement results.
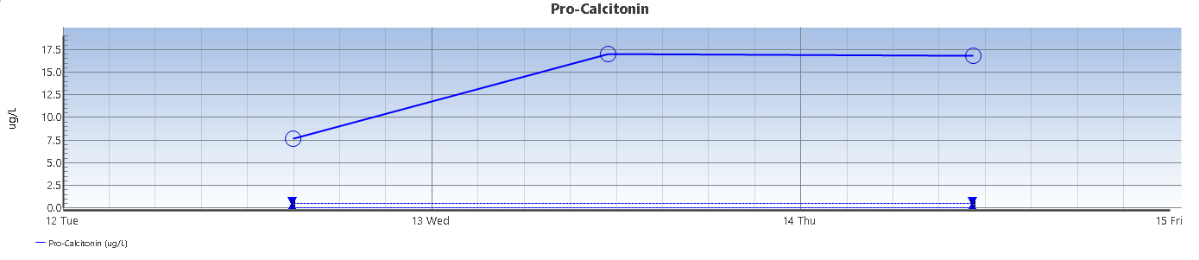
Figure 5: Pro-calcitonin level measurement results.
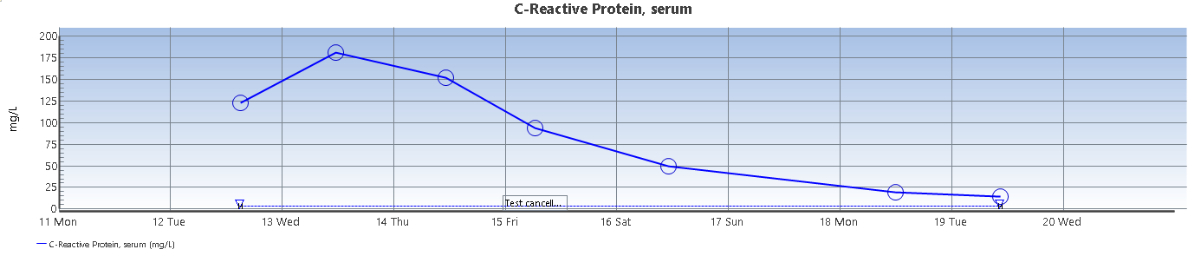
Figure 6: C-reactive protein level measurement results.
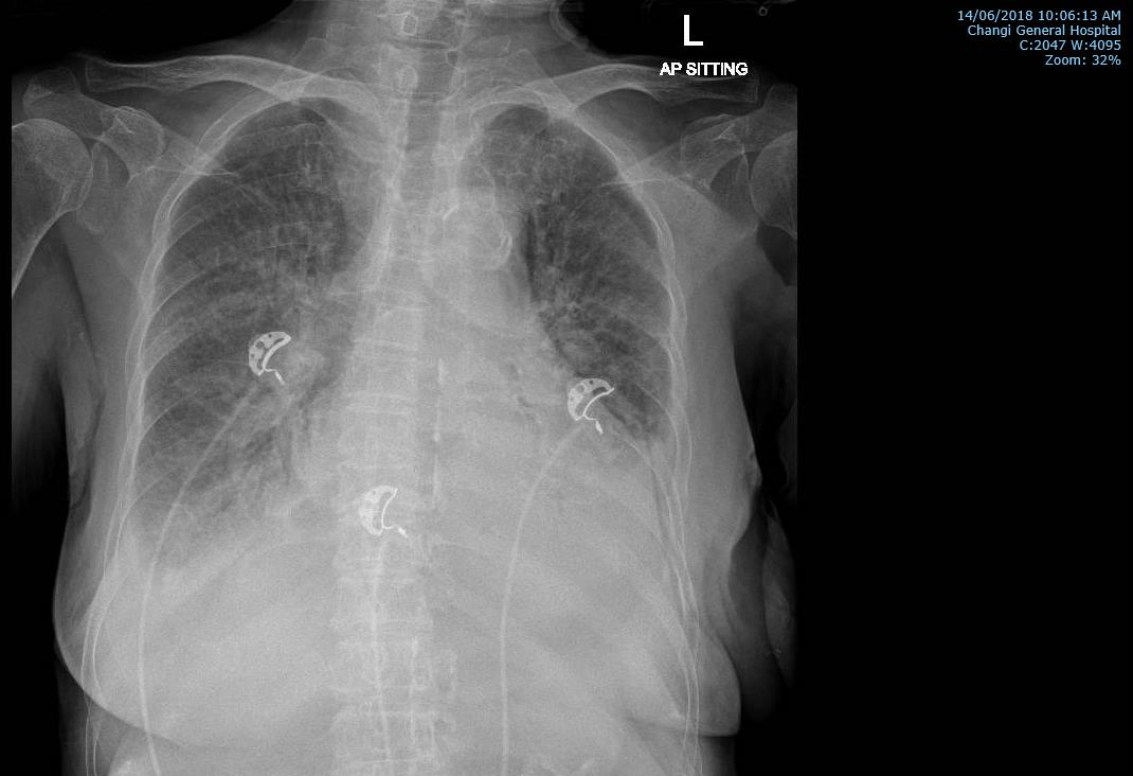
Figure 7: Chest x-ray radiograph after 2 days of treatment in the ward.
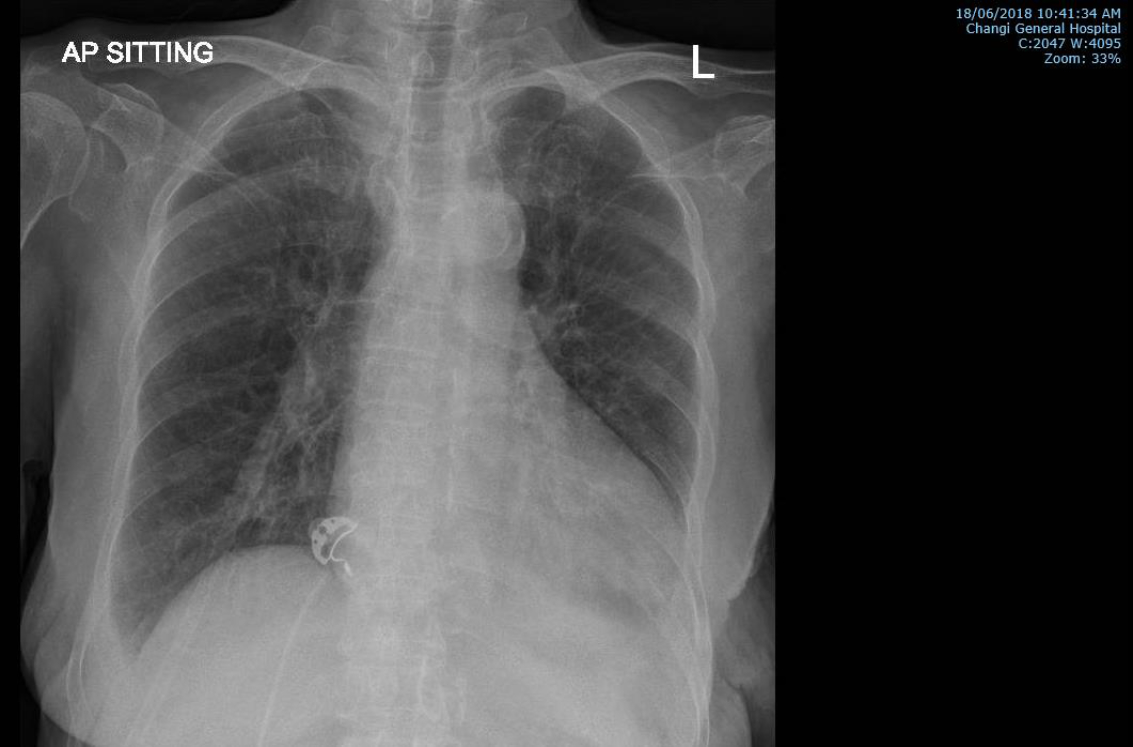
Figure 8: Chest x-ray radiograph after 4 days of treatment in the ward.
5. Outcome and Follow-up
Patient continued to improve with the above management and future plan is to switch to oral diuretics once the dry weight of the patient is achieved and symptoms resolved.
6. Discussion
Clinical conditionin which dysfunction and bidirectional injury of both kidney and heart are present is called cardio-renal syndrome (CRS) [1]. Acute cardio-renal syndrome or type 1 CRS is acute worsening of heart function giving rise to acute kidney injury (AKI). Among inpatients with acute decompensated heart failure (ADHF), 25% of them have type 1 CRS [2]. Interestingly, a study in Chinese elderly patients ≥60 years old showed higher incidence of type 1 CRS, which is 52.56% [3].
Several factors may contribute to the higher prevalence of type 1 CRS in elderly patients. The factors include more exposure to nephrotoxins and chronic diseases, as well as an increase in the number of chronic and comorbid diseases [3]. In type 1 CRS, a decrease in renal blood flow and subsequent reduction of glomerular filtration rate (GFR) are the major haemodynamic mechanisms. Non-haemodynamic mechanisms may also be involved including renin angiostensin-aldosterone system (RAAS) and sympathetic nervous system activation, chronic inflammation, and change in reactive oxygen species (ROS)-nitric oxide (NO) production ratio. Perpetuating case of AKI can be due to endothelial cell death and renal ischemia-induced apoptotic mechanism leading to structural and functional loss of epithelial cells. Cellular damage of the renal tubule is strongly associated with renal cell apoptosis and intra-renal inflammatory activity [2].
In acute cardio-renal syndrome or type 1 CRS, the timing of development of AKI is mostly within 48 hours of onset of ADHF [2]. In this patient case, AKI is observed on the third day of ADHF presentation. Only eight percent of AKI developed on day 3 and same percentage also applies to the AKI development on day 4 [2]. According to KDIGO Clinical Practice Guideline for Acute Kidney Injury, the diagnosis of stage 1 AKI can be made according to serum creatinine level and/or urine output status. Stage 1 AKI is the condition in which serum creatinine level is elevated by ≥0.3 mg/dl (26.5 μmol/L) within 48 hours, or when within 6-12 hours the urine output is reduced to <0.5 mL/kg/h [4]. KDIGO criteria may be used as identification and short-term prognosis prediction tools in the case of type 1 CRS. Compared with RIFLE and AKIN criteria, KDIGO criteria also significantly identify more type 1 CRS episodes [5].
Recent studies showed that many possible protein biomarkers may be useful in type 1 CRS. A promising diagnostic marker neutrophil gelatinase-associated lipocalin (NGAL) may be used owing to its 100% sensitivity and 86.7% specificity in detecting CRS type 1 (n=119). Despite its sensitivity and specificity, another study involving 927 hospitalised patients showed that NGAL could not detect worsening renal function better than creatinine. Among 166 patients in another study, a gromerular filtration and integrity marker Cystatin-C was an independent predictor of worse renal function in inpatients with type 1 CRS. Evidence also showed prognostic value of n-acetyl-beta-D-glucosaminidase (NAG), proenkephalin, and kidney injury molecule-1 (KIM-1) for AKI/CKD in CRS patients. However, many studies utilised different definition for type 1 CRS [6]. It is suggested that globally accepted criteria for type 1 CRS should be established and subsequent meaningful clinical trials should be conducted with larger sample size for early type 1 CRS detection and hence successful treatment.
Improvement of renal function from therapeutic interventions may be advantageous in type 1 CRS case [7]. It is achievable by reducing congestion with diuretics and balancing this with the rate of intravascular refilling from the interstitial space [8]. The “5B” approach can be considered for the management and consists of:
- Balance of fluids reflected by body weight
- Blood volume
- Blood pressure
- Biomarkers
- Bioimpedance vector analysis [9].
In elderly patients of Chinese population with type 1 CRS, beta-blocker and diuretics administration are protective factors, although diuretics use is also a risk factor to incidence of this type of CRS [3]. The treatment for this condition is also still far from been standardised [10]. Nevertheless, diuretics remain the mainstay of treatment until safer and more effective alternatives are found [11]. The most commonly used diuretic drug for volume overload treatment is furosemide. In terms of drug administration, intravenous infusion is preferred on account of poor absorption of oral furosemide in view of gut hypoperfusion and oedema. However, diuretic resistance may ensue from the pharmacokinetics of furosemide [10][12]. In low output states inotropes can be considered for treatment. On the other hand, empiric vasodilators may be needed in the type 1 CRS with preserved or elevated blood pressure [6].
Patients admitted due to heart failure who experience worsening renal function have poor prognosis [7]. Glomerular filtration is also decreased in the presence of diabetes and presentation [12], both of which were present in the case report patient. As GFR declines and anaemia is present, mortality increases and hospital stay is prolonged [7][11]. Among nearly 50,000 patients with heart failure involved in OPTIMIZE-HF registry, 51% of them had haemoglobin ≤12g/dL. In those with heart failure and concomitant kidney disease, erythropoietin level may be low. Correction of anaemia in patients with heart failure however requires caution on grounds of the association between aggressive anaemia correction and increased rate of adverse events in this patient population [11].
7. Conclusion and Recommendations
- A higher incidence rate of type 1 CRS was seen in Chinese elderly population
- Observation of AKI especially during the first 48 hours after onset of ADHF is crucial in order to make early diagnosis and to treat the condition.
- The “5B” approach can be considered for the management of the clinical condition with diuretics being the common mainstay of treatment.
- Globally agreed criteria for type 1 CRS should be established prior to meaningful clinical trials in this field.
8. References
[1] McCullough PA, Ahmad A. Cardiorenal syndromes. World J Cardiol. 2011 Jan 26; 3(1): 1-9.
[2] Di Lullo L, Bellasi A, Barbera V, Russo D, Russo L, Di Iorio B, Ronco C. Pathophysiology of the cardio-renal syndromes types 1-5: An uptodate. Indian Heart J. 2017 Mar – Apr; 69(2): 255-65.
[3] Hu W, He W, Liu W, Fang X, Wu Y, Yu F, Hao W. Risk Factors and Prognosis of Cardiorenal Syndrome Type 1 in Elderly Chinese Patients: A Retrospective Observational Cohort Study. Kidney Blood Press Res. 2016; 41(5): 672-9.
[4] KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int Suppl 2012; 2:8.
[5] Li Z, Cai L, Liang X, Du Z, Chen Y, An S, Tan N, Xu L, Li R, Li L, Shi W. Identification and Predicting Short-Term Prognosis of Cardiorenal Syndrome Type 1: KDIGO Is Superior to RIFLE or AKIN. PLoS One. 2014; 9(12): e114369.
[6] House AA, Haapio M, Lassus J, Bellomo R, Ronco C. Pharmacological Management of Cardiorenal Syn- dromes. Int J Nephrol. 2011; 2011: 630809.
[7] Gottlieb SS, Abraham W, Butler J, Forman DE, Loh E, Massie BM, O’connor CM, Rich MW, Stevenson LW, Young J, Krumholz HM. The prognostic importance of different definitions of worsening renal function in congestive heart failure. J Card Fail. 2002 Jun; 8(3): 136-41.
[8] Ronco C, Kaushik M, Valle R, Aspromonte N, Peacock WF 4th. Diagnosis and management of fluid overload in heart failure and cardio-renal syndrome: the “5B” approach. Semin Nephrol. 2012 Jan; 32(1): 129-41.
[9] Petra E, Zoidakis J, Vlahou A. Protein biomarkers for cardiorenal syndrome. Expert Rev Proteomics. 2019 Apr; 16(4): 325-36.
[10] Cice G. Renal insufficiency in acute heart failure: old habits we need to let go? Eur Heart J Suppl. 2019 Mar; 21(SupplB): B38-B42.
[11] Bock JS, Gottlieb SS. Cardiorenal syndrome: new perspectives. Circulation. 2010 Jun 15; 121(23): 2592- 600.
[12] Liu PP. Cardiorenal syndrome in heart failure: A cardiologist’s perspective. Can J Cardiol. 2008 Jul; 24(Suppl B): 25B-29B.
Article photo credit: John Campbell
- Log in to post comments










