In children in the care system, how can we improve mental health services for the treatment of mental health disorders in this paediatric subpopulation?

1. Introduction
Recent research indicated that the prevalence of mental health disorders among children and adolescents had significantly increased over the last few years [1][2]. A recent systematic review and meta-analysis by Bronsard et al. 2016, assessed the prevalence of mental health disorders among ‘children in care’, and found higher incidences of mental health disorders among this paediatric subgroup. In this article, ‘children in care’ referred to children under the age of eighteen years old, in foster care and out-of-home placement such as within institutions and hospitals. Many of these children have had traumatic family histories and life experiences, including histories of child abuse and neglect, abandonment and household instability, which resulted in their reported increased mental health incidence and delinquent behaviour. Both the health and societal implications therefore highlighted the urgent need to improve the access and quality of mental health services for the treatment of mental health disorders amongst children in care. Therefore, it would be interesting to see how children in the care system’s treatment needs could be better met under the current NHS system. However, the main concern was how to approach such a question. Mental health conditions which appeared quite frequent in the child and adolescent populations included depression, anxiety and conduct disorders [1]. These mental health conditions were treatable, and the management had adopted an evidence-based medicine approach [3]. First-line treatment included psychological interventions and progressed to a combination of psychological and pharmacological interventions for moderate to severe cases. For instance, the NICE guidelines for depression recommended the first-line treatment to be psychotherapy such as Cognitive Behavioural Therapy (CBT). However, when psychotherapy was unavailable or ineffective, Fluoxetine was recommended for the treatment of moderate to severe depression. A number of lessons could be learnt from the current management guidelines for the treatment of mental health disorders in the general child and adolescent population. However, it was more important to recognise that the guidelines for the treatment of mental health disorders have been subject to a significant amount of scrutiny itself [4]. Many of the studies which have assessed this area have a number of methodological flaws, including selective reporting, publisher bias, and the ‘Placebo Effect’ – the beneficial act of merely prescribing a pill and should be taken into consideration for this review [5]. The objectives of this study were to analyse the literature surrounding the access and quality of mental health services amongst children and adolescents, and where possible amongst children in care. Secondly, it explored the important factors responsible for the efficacy of treatment interventions, with efficacy determined by reduced mental health disorders and hospitalisation rates. Thirdly, it assessed whether these findings could then be extrapolated and utilised for the purposes of improving the mental health services for children and adolescents in the care system.
2. Methodology
2.1 Search strategy An update of the literature surrounding psychiatric services in children’s mental health was conducted and only the highest level of evidence of published systematic reviews, meta-analyses and primary data was located. The Cochrane and Pubmed databases were searched, for articles published up until 9th January 2018. The exact search strings used were summarised in Appendix 1. 2.2 Selection criteria The inclusion criteria were: (i) published in a peer-reviewed journal; (ii) examined mental health service in children and adolescents with mental health disorders, ideally in care; (iii) provided a measure or the means to measure the quality, access or efficacy of mental health services (iv) controlled study or pooled patient-level systematic review or meta-analysis; and (v) in English. Exclusion criteria were (i) publication which was not primary or pooled research e.g. comment, editorial, letter (ii) study which did not report on the quality, access or efficacy of the mental health service and (iii) duplication of previously published data. 2.3 Data extraction Full-text review of articles was conducted by one independent investigator, using the above criteria. Eligibility decisions and disagreements were reconciled via reanalysis of the inclusion and exclusion criteria. Data were extracted using a form with pre-populated headings based on the study group, study type, data collection and key findings, to minimise data interpretation bias.
3. Results
Of the 1,309 unique citations screened, 1, 298 articles were excluded at the title and abstract level based on the inclusion/exclusion criteria. A significant proportion of the articles were manually excluded, as a consequence of increasing the sensitivity of the search strategy to incorporate for all the substitutions of the word ‘child.’ A further 5 were excluded after full-text assessment. The most common reasons for exclusion included the lack of measure or the means to measure the quality, access or efficacy of the mental health service. For this particular review, seven studies relevant to child and adolescent psychiatry and psychiatric services were identified (Fig. 1).
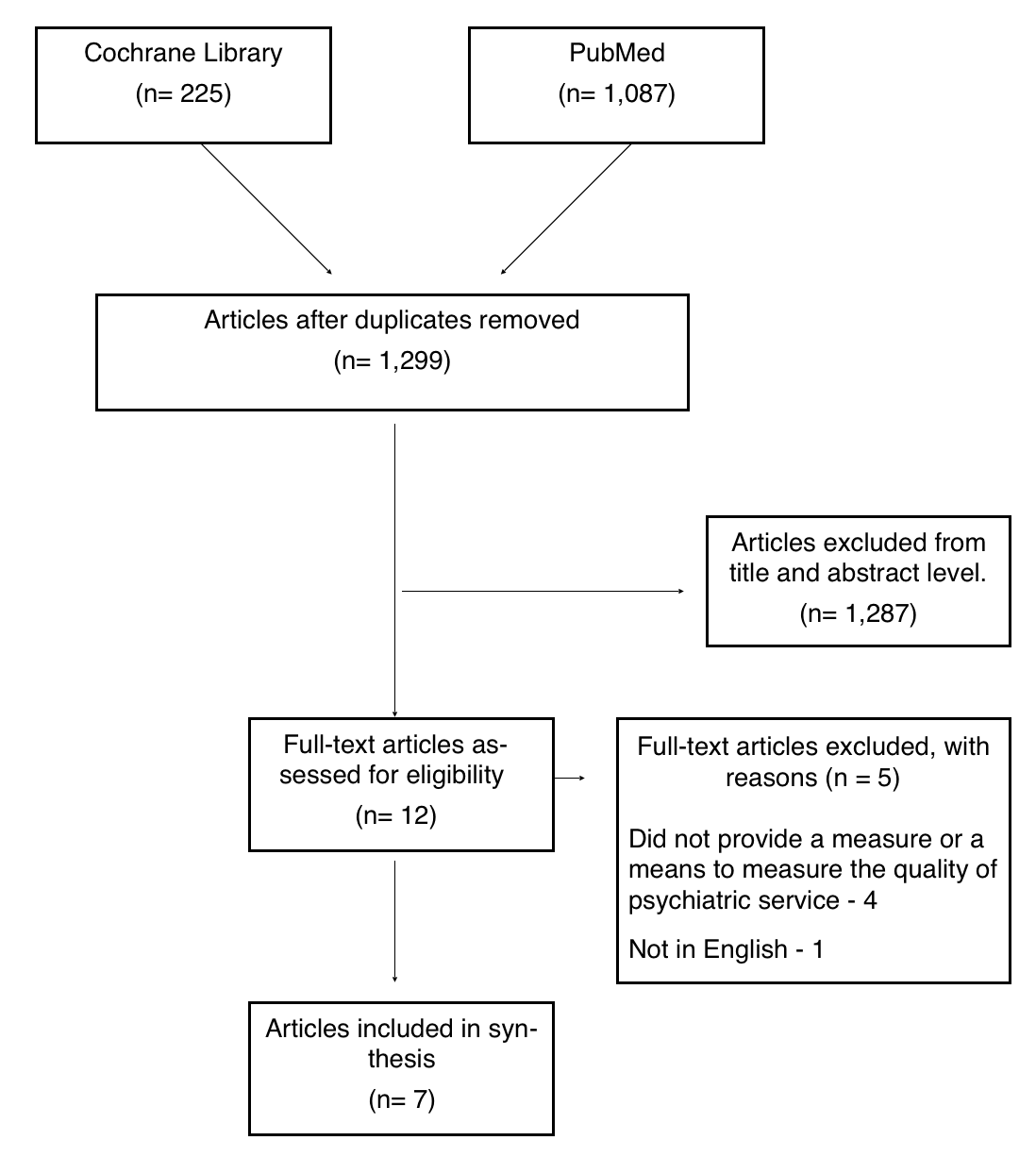
Figure 1: PRISMA Flow diagram for selection of articles on children and adolescent psychiatry.
4. Discussion
This review identified seven studies on mental health services amongst children and adolescents. The findings were in keeping with the current literature stating that children in care had disproportionately high rates of emotional and behavioural disorders, including depression, anxiety, substance abuse and criminality, compared to children who were not in care [1]. Reasons for the increased incidence have been linked to childhood traumatic experiences, such as abandonment, serious neglect or maltreatment. Childhood traumatic experiences have consequently been associated with long-term adverse outcomes such as delinquency and involvement with the criminal justice system [6]. The first objective was to assess the access and quality of psychiatric services amongst children and adolescents. There appeared to be a significant degree of variation between the quality of services within studies. This was complicated by the variability in the service needs of children and adolescents of different genders, ages and psychiatric conditions [7][8][9][10][11][12]. Mental health conditions also tended to co-occur, such as depression and generalised anxiety disorder and the stigma associated with mental health interfered with patient compliance. Moreover, there was a general lack of developmentally appropriate services for youth. Therefore the first recommendation that should be made would be to train service providers in the different mental health conditions that affect children and adolescents of different age groups and genders, thereby allowing psychiatric services to facilitate the current needs of the child or adolescent. In terms of access to Child and Adolescent Mental Health Services, the waiting time could be up to 18 weeks and in some areas even more [14]. The waiting time can be ameliorated by investing more funds to train and recruit more staff whom can provide the services. Another complication that resided within the literature was that many of the studies included in the reviews or studies themselves were subject to a number of methodological flaws, including publisher bias, selective reporting, non-blinding and low-power such as the discrepancies between the effectiveness of antidepressants in adolescent depression [4][5]. Some studies found no statistically significant difference between antidepressants and placebo, whilst others did indicate a difference and these variations were in part due to the methodological flaws the studies were vulnerable to. However, in terms of specific interventions, either antidepressant or psychological therapies were found to be efficacious for anxiety, depressive and co-morbid disorders compared to the placebo [8][9][11]. Table 1: Summary of evidence.
| CITATION | STUDY GROUP | STUDY TYPE | OUTCOME | KEY RESULTS | COMMENTS |
|---|---|---|---|---|---|
| Carney et al., 2016 [7] | 6 studies with 1176 adolescents comparing brief,interventions with information provision only or with assessment only. | A structured, systemic review of evidence-based interventions for substance-using adolescents. | 1. Reduction,or cessation of substance use. 2. Engagement in criminal activity or delinquent problem behaviours related to,substance use. | 1. When compared to information provision, brief interventions were not more efficacious in reducing substance use. When compared to assessment-only controls, it was found to significantly reduce the frequency of alcohol abuse and dependence, and cannabis abuse, in some studies. 2. When compared to information provision, brief interventions had no significant effect on delinquent behaviour and resulted in mixed effects on adolescents’ delinquent or problem behaviour. When compared to assessment-only, brief interventions resulted in an improvement in delinquent or problem behaviours at long-term follow-up. | Brief, school-based interventions for the treatment of substance abuse were efficacious,compared to assessment. This article also did not address children in the care,system specifically. However, limitations included lack of power from small sample sizes, no blinding,and no concealment of group allocation, therefore difficult to conclude the efficacy,of brief interventions. |
| Cox et al., 2014 [8] | 11 studies with 1307 children or adolescents, with,different severities of disorder and variety of co-morbid disorders. | Structured, systematic review of the efficacy of psychological therapies and antidepressant medication, alone and in combination. | 1. Comparison of the efficacy of antidepressant medication compared to psychotherapy on remission immediately post-intervention, in terms of several clinical outcomes, including clinical and self-reported depression measures, suicide-related outcomes. 2. Comparison of combination therapy to antidepressant medication alone on remission immediately post-intervention. 3. Comparison of combination therapy to psychological therapy alone on remission immediately post-intervention | 1. Odds Ratio (OR) 0.52 95% Confidence Interval,(CI) 0.27-0.98. 2. OR 1.56, 95% CI 0.98-2.47 3. OR 1.82, 95% CI 0.38-8.68. | Generally, there was limited evidence regarding the effectiveness of one intervention over another, compared to a combination of these interventions. One intervention did not appear to be superior to the other. A combination of treatment interventions was reported to provide both a faster treatment response and protection against suicidality, compared to medication or psychological intervention alone. Limitations to this study included lack of power, randomisation, adequate allocation, concealment and blinding. |
| Hawkins, 2009 [9] | 23 studies on adolescents with co-occurring disorders, and co-occurring disorder treatment models. | A systematic review of co-occurring disorders among adolescents, treatment models and outcomes. | Provide a better understanding and overview of issues surrounding cooccurring disorders among adolescents, general treatment considerations, selected treatment models and outcomes, and presentation,of recommendations and best practice strategies. | 1. Co-occurring disorders among adolescents were very common, with the highest rate of co-occurring substance use disorders among youth with disruptive behaviour disorders. 2. Adolescents with co-occurring disorders often failed to receive effective treatment, due to the associated stigma, lack of developmentally appropriate service for youth, and lack of funding. 3. Some treatment models showed positive outcomes e.g. Child and Youth Intensive Case, as they focussed on a particular area such as treatment planning and care coordination. This led to a reduction in hospital rates and duration, increase in days spent in the community, a decrease in symptoms and higher functioning levels. | Mental health disorders often co-occurred and varied in their severity and subtype. Comprehensive integrated service system has been the most efficacious in the treatment of adolescents with co-occurring disorders. This is where services worked together, and there,were individuals coordinating and specialised to deal with the complex needs of adolescents. |
| Hetrick et al, 2016 [10] | Randomised Controlled Trial (RCT) with 500 youth presenting for hospital-based outpatient psychiatric service. | RCT in partnership with 4 community agencies, 4 adolescent psychiatry hospital departments, youth and family members with lived experience of mental health access service use, and other stakeholders. | 1. Youth’s functioning at intake, 6 months and 12 months following treatment. 2. Intent-to-treat analyses will be used on repeated measures data, along with cost-effectiveness and cost-utility analyses, to determine intervention effectiveness | 1. Risk Difference RD, -0.03, 95% Confidence Interval, -0.05 – -0.01. The risk of having a diagnosis of depression was reduced for participants receiving intervention compared to no intervention. This effect persisted for up to 12 months. 2. Estimates of numbers needed to treat to benefit (NNTB = 11) compared well with other public health interventions. The results showed small positive benefits of depression prevention. | The model used in the treatment of mental health disorders in this study showed promise. The advantages of the model were the involvement of youth, family members and other stakeholders through all phases of the project, and it was tailored to the needs, goals and preferences of the patient. Interventions delivered to targeted populations, particularly those selected on the basis of depression symptoms, had larger effect sizes. Limitations included lack of concealment and blinding. |
| Ipser et al., 2009 [11] | 22 Randomised Controlled Trials (RCT) with 2519 participants, assessing the efficacy of medication for treating paediatric anxiety disorders. | A systematic review of the efficacy and tolerability of medication for treating paediatric anxiety disorders, mainly SSRIs. | 1. Treatment response in the medication group to the placebo group, as determined by the Clinical Global Impressions scale (CGI-I), and anxiety symptoms. 2. A response of comorbid symptoms to medication, quality of life measures & acceptability of medication. | 1. Relative Risk (RR) 1.9, 95% Confidence Interval (CI) 1.6-2.26. Treatment response was significantly greater. 2. There was an improvement in the quality of life as a result of the medication but not other factors. | Medication was more effective than placebo in reducing overall symptoms severity across all of the anxiety disorders, and children responded better to the antidepressants (mainly SSRIs) than no treatment. However, there were more withdrawals from the medication group, due to drug-related adverse events, and hence the study was limited by potential biases from the high withdrawal rate and lack of concealment. Overall, there is no clear evidence to show that any particular class of medication was more effective or better tolerated than any other, and more evidence would be required on the long-term efficacy of medication treatment and optimal dosages. |
| Larun et al., 2006 [12] | 16 Randomised Controlled Trials (RCTs) with 1191 participants between 11 and 19 years. | A systematic review assessing the effects of exercise interventions in reducing or preventing anxiety or depression in children and young people up to 20 years of age. | 1. Reduction/prevention of anxiety/depression among children and young people compared to no/other treatments. 2.Characteristics of the most effective interventions. 3. Prevalence of anxiety or depression. | 1. Exercise reduced depression and anxiety scores in the general population of children and young people. 2. There was little difference between whether the exercise was of high or low intensity when vigorous exercise was compared to low-intensity exercise. 3. Prevalence rates were not reported. | Exercise may be effective in the reduction or prevention of anxiety or depression. Exercise, lifestyle modifications and self-regulation are all important. However, their role should be explored further with good quality randomised controlled trials, to determine their efficacy in the psychiatric service of paediatric and adolescent patients. Limitations included the use of studies of low methodological quality. |
| Sakair, Lin, Flores, 2011 [13] | Cohort study with 1308 participants entering out-of-home care following reported maltreatment. | 3-year cohort study examining health outcomes and family services in kinship care. | Baseline caregivers’ support services and the children’s behavioural, mental health, and health service use outcomes 3 years after placement. | 572/1308 children were in kinship care and 736/1308 children were in foster care. Children in kinship care were more likely to than children in foster care to have a permanent caregiver, and had 0.6 times the risk of behavioural problems and social skills problems, but had 7 times the risk of pregnancy and 2 times the risk of substance use. The rates of clinical depression and post-traumatic stress disorder did not significantly differ between the 2 groups. | Permanent caregivers played an important role in the incidence,of mental health problems in children and adolescents.\linebreak{} It was interesting to see the lower prevalence of risk-taking behaviours in foster,care e.g. fewer pregnancies, suggesting the possible benefits of the care system,,such as the higher degree of agency and caregiver supervision. |
Exercise and brief interventions may reduce anxiety and depression symptoms or substance abuse respectively but the evidence remained inconclusive [7][12]. The role of lifestyle modifications, exercise and self-regulation should also be explored further to determine their efficacy in the treatment of paediatric and adolescent patients [8][11][12]. The second objective was to determine the factors responsible for the efficacy of treatment interventions. Efficacy was determined by a reduction in mental health disorders, hospitalisation rates or improvements in symptoms or compliance to the service [9][10][13]. These factors included early intervention, treatment planning appropriate to the individual and subsequent coordination of care services between service providers. Therefore, I would advise the development of psychiatric services which considered the above factors. It would also be important to address patient compliance with psychiatric services and thereby stress the importance of maintaining health and wellbeing and dissipate the stigma associated with mental health conditions. Another recommendation to improve mental health services would be to assess the level of support required for a particular foster family and provide the required support, encouragement, and education for caring for a child with a mental health disorder. This can also be easily incorporated into current educational programs provided to foster carers by some trusts, such as the Cambridgeshire and Peterborough NHS Trust [15]. The third objective was to assess whether these findings could be extrapolated to children and adolescents in the care system. The real difficulty, which remained with this research question was being able to identify studies which reported the access, quality or efficacy of psychiatric services amongst children in care. Unfortunately, there were very few studies on children in care and even fewer still on the management and treatment of this group, as it was a difficult group to target. Hence, why it was important to assess the lessons learnt from the management of the general paediatric population and examine the provisions that could be in place for children in the care system. Evidence suggested that some of the factors which precipitated children in the general paediatric population to develop mental health disorders were similar to children in foster care [16]. Therefore, the results, such as the need to improve early access and intervention, amongst other recommendations, could be applied to children in the care system. However, it would be important to identify the risk factors during the assessment and thereby ensure children in care are receiving the appropriate treatment. Further studies I would recommend include more primary studies assessing the quality, access or efficacy of psychiatric services amongst children in the care system, for treatment purposes, and an assessment of the effectiveness of some of the novel psychiatric service models [9][10] described in the review on a larger sample size.
5. Appendices
Appendix 1. Search strategy and systematic review of searches in Cochrane Library and Pubmed Key words developed from brainstorming, synonyms, MeSH words, using search options, referral to other articles’ ap-pendices on children in care, mental health services and mental health disorders, using the Cochrane database, and checking their list of key words against mine. The last date searched was 9th January 2018. PubMed searches: (https://www.ncbi.nlm.nih.gov/pubmed)
- “foster child*” OR “child* in care” OR “foster care child*” OR “child* in out-of-home care” OR “out-of-home care child*” OR “child* in substitute care” OR “substitute care child*”
- “foster girl*” OR “girl* in care” OR “foster care girl*” OR “girl* in out-of-home care” OR “out-of-home care girl*” OR “girl* in substitute care” OR “substitute care girl*”
- “foster boy*” OR “boy* in care” OR “foster care boy*” OR “boy* in out-of-home care” OR “out-of-home care boy*” OR “boy* in substitute care” OR “substitute care boy*”
- “foster teen*” OR “teen* in care” OR “foster care teen*” OR “teen* in out-of-home care” OR “out-of-home care teen*” OR “teen* in substitute care” OR “substitute care teen*”
- “foster adolescent*” OR “adolescent* in care” OR “foster care adolescent*” OR “adolescent* in out-of-home care” OR “out-of-home care adolescent*” OR “adolescent* in substitute care” OR “substitute care adolescent*”
- #1 OR #2 OR #3 OR #4 OR #5
- “psychiatr* service use” OR “psychiatr* service utilisation” OR “mental health service use” OR “mental health service utilisation” OR “health service use” OR “health service utilisation” OR “help-Seeking”
- “mental disorder*” OR “mood disorder*” OR “personality disorder*” OR “schizophrenia and disorders with psy-chotic features” OR “anx*” OR “depress*” OR “panic*” OR “obsess*” OR “OCD” OR “substance*”
- #6 AND #7 AND #8
Search Results: 1087 results, 1080 did not meet the inclusion criteria. Cochrane Library searches: (http://www.cochranelibrary.com)
- “foster child*” OR “child* in care” OR “foster care child*” OR “child* in out-of-home care” OR “out-of-home care child*” OR “child* in substitute care” OR “substitute care child*” OR “foster girl*” OR “girl* in care” OR “foster care girl*” OR “girl* in out-of-home care” OR “out-of-home care girl*” OR “girl* in substitute care” OR “substitute care girl*” OR “foster boy*” OR “boy* in care” OR “foster care boy*” OR “boy* in out-of-home care” OR “out-of-home care boy*” OR “boy* in substitute care” OR “substitute care boy*” OR “foster teen*” OR “teen* in care” OR “foster care teen*” OR “teen* in out-of-home care” OR “out-of-home care teen*” OR “teen* in substi-tute care” OR “substitute care teen*” OR “foster adolescent*” OR “adolescent* in care” OR “foster care adoles-cent*” OR “adolescent* in out-of-home care” OR “out-of-home care adolescent*” OR “adolescent* in substitute care” OR “substitute care adolescent*”
- AND “psychiatr* service use” OR “psychiatr* service utilisation” OR “mental health service use” OR “mental health service utilisation” OR “health service use” OR “health service utilisation” OR “help-Seeking”
- AND “mental disorder*” OR “mood disorder*” OR “personality disorder*” OR “schizophrenia and disorders with psychotic features” OR “anx*” OR “depress*” OR “panic*” OR “obsess*” OR “OCD” OR “substance*”
- Limits: Record Title
Search Results: 225 results, 221 did not meet the inclusion criteria.
6. References
[1] Bronsard, G., Alessandrini, M., Fond, G., Loundou, A., Auquier, P., Tordjman, S. and Boyer, L. (2016). The Prevalence of Mental Disorders Among Children and Adolescents in the Child Welfare System. Medicine, 95(7), p.e2622. [2] Pecora PJ, Jensen PS, Romanelli LH, Jackson LJ, Ortiz A (2009) Mental Health Services for Children Placed in Foster Care: An Overview of Current Challenges. Child Welfare. 88(1):5-29 [3] Nice.org.uk. (2018). Depression in children and young people: identification and management | Guidance and guidelines | NICE. [online] Available at: https://www.nice.org.uk/guidance/cg28 [Accessed 1 May 2018]. [4] Hetrick, S. E., McKenzie, J. E., Cox, G. R., Simmons, M. B., & Merry, S. N. (2012). Newer generation antidepressants for depressive disorders in children and adolescents. Cochrane Database of Systematic Reviews, (11). https://doi.org/10.1002/14651858.CD004851.pub3 [5] Bridge, J. A., Birmaher, B., Iyengar, S., Barbe, R. P., & Brent, D. A. (2009). Placebo response in randomized controlled trials of antidepressants for pediatric major depressive disorder. The American Journal of Psychiatry, 166(1), 42-49. https://doi.org/10.1176/appi.ajp.2008.08020247 [6] Fratto CM [7] Carney T, Myers BJ, Louw J, Okwunda CI (2016) Brief school-based interventions and behavioural outcomes for substance-using adolescents (Review). Cochrane Database of Systematic Reviews. 20;(1):CD008969 [8] Cox GR, Callahan P, Churchill R, Hunot V, Merry SN, Parker AG, Hetrick SE (2014) Psychological therapies versus antidepressant medication alone and in combination for depression in children and adolescents (Review). Cochrane Database of Systematic Reviews. 11:CD0083242 [9] Hawkins EH (2009) A Tale of Two Systems: Co-Occurring Mental Health and Substance Abuse Disorders Treatment for Adolescents. Annual Review of Psychology. 60:197-227 [10] Hetrick SE, Cox GR, Witt KG, Bir JJ, Merry SN (2016) Cognitive behavioural therapy (CBT), third-wave CBT and interpersonal therapy (IPT) based interventions for preventing depression in children and adolescents (Review). Cochrane Database Systematic Review. 9(8): CD003380 [11] Ipser JC, Stein DJ, Hawkridge S, Hoppe L (2009) Pharmacotherapy for anxiety disorders in children and adolescents (Review). Cochrane Database Systematic Review. 8;(3):CD005170. [12] Larun L, Nordheim LV, Ekeland E, Hagen KB, Heian F (2006) Exercise in prevention and treatment of anxiety and depression among children and young people (Review). Cochrane Database Systematic Review. 19;(3):CD004691. [13] Sakai C, Lin H, Flores G (2011) Health Outcomes and Family Services in Kinship Care. Arch Pediatr Adolesc Med. 165(2):159-165 [14] Smith, J., Kyle, R., Daniel, B. and Hubbard, G. (2017). Patterns of referral and waiting times for specialist Child and Adolescent Mental Health Services. Child and Adolescent Mental Health, 23(1), pp.41-49. [15] Peterborough City Council. (2018). Children in care. [online] Available at: https://www.peterborough.gov.uk/healthcare/childrens-social-care/children-in-care/ [Accessed 1 May 2018]. [16] Mental Health Foundation. (2018). Lifetime Impacts. [online] Available at: https://www.mentalhealth.org.uk/publications/lifetime-impacts [Accessed 1 May 2018]. Article photo credit: netzanette
- Log in to post comments










